How To Detect Bunions
Overview
 Bunions (sometimes referred to as Hallux abducto valgus) are enlargements of the inner portion of the metatarsophalangeal (MTP) joint at the base of your big toe. More commonly, they are described as a bump on the side of the big toe. The foot bunion is the result of changes that occur in the framework of the bones at the front of your foot. Instead of pointing straight ahead, your big toe begins to lean into your second toe, throwing the bones out of alignment. Bunions are progressive, meaning you will not just wake up one day and find a visible bump (unless it was caused by a bug bite or something of that nature). Bunions are generally attributed to genetics and improper footwear. It may take years for a bunion to fully develop and begin to show symptoms. Some people may never experience symptoms at all. Bunions may begin to form during one?s teenage years, but they usually occur in people aged 20-30. Women are three times more likely than men to have bunions.
Bunions (sometimes referred to as Hallux abducto valgus) are enlargements of the inner portion of the metatarsophalangeal (MTP) joint at the base of your big toe. More commonly, they are described as a bump on the side of the big toe. The foot bunion is the result of changes that occur in the framework of the bones at the front of your foot. Instead of pointing straight ahead, your big toe begins to lean into your second toe, throwing the bones out of alignment. Bunions are progressive, meaning you will not just wake up one day and find a visible bump (unless it was caused by a bug bite or something of that nature). Bunions are generally attributed to genetics and improper footwear. It may take years for a bunion to fully develop and begin to show symptoms. Some people may never experience symptoms at all. Bunions may begin to form during one?s teenage years, but they usually occur in people aged 20-30. Women are three times more likely than men to have bunions.
Causes
Bunions tend to run in families, although it is the faulty foot mechanics that lead to bunions that are inherited, not the bunions themselves. Some authorities, in fact, suggest that the most significant factor in bunion formation is the poor foot mechanics passed down through families. However, the American Orthopaedic Foot and Ankle Society estimates that women have bunions nine times more often than men, that 88 percent of women in the United States wear shoes that are too small, and that 55 percent of women have bunions. Again, this reflects the wearing of shoes with tight, pointed toes, or with high heels that shift all of your body's weight onto your toes and also jam your toes into your shoes' toe boxes. It should be noted that it generally takes years of continued stress on the toes for bunions to develop.
Symptoms
Signs and symptoms of a bunion include the base of the big toe is swollen and sticks out. The big toe is often bent towards the other toes, and sometimes the second toe is pushed to overlap the third toe. Skin around the big toe joint is red and sore. Thickened skin at the base of the big toe. Pain in the big toe or foot. Wearing shoes is painful. Pain or difficulty when walking.
Diagnosis
The doctor considers a bunion as a possible diagnosis when noting the symptoms described above. The anatomy of the foot, including joint and foot function, is assessed during the examination. Radiographs (X-ray films) of the foot can be helpful to determine the integrity of the joints of the foot and to screen for underlying conditions, such as arthritis or gout. X-ray films are an excellent method of calculating the alignment of the toes when taken in a standing position.
Non Surgical Treatment
Long-term treatment of bunions must be directed towards re-balancing the foot, so that we no longer walk with our weight forced on to the inner border of the foot. This is accomplished by controlling and reducing pronation with the use of a high quality arch support or custom made orthotics. These devices comfortably re-balance the feet and overcome pronation. This reduces the abnormal weight forces on the big toe and its metatarsal head, allowing the feet to function normally. As a result, the deformity should not worsen, and the pain should gradually subside. If the foot is not re-balanced, the deformity and pain will become worse. 
Surgical Treatment
Bunion surgery can be performed under local or general anaesthetic. The operation usually takes between half an hour to an hour. There are several types of bunionectomies. Some involve removal and realignment of the bones in your foot. Mild bunion problems can sometimes be resolved using soft tissue release or tightening. For some very severe cases bones of the big toe are fused or the bunion is cut out along with some of the bone at the base of the toe. Be sure and discuss which type of operation you will have with your surgeon. With any type of bunionectomy your surgeon will make one or more incisions (cuts) near your big toe. They will use instruments to trim the bones and remove the bunion. Wire, screws or plates may also be used to hold the new joint in place.
How To Tell If I'Ve Got Over-Pronation Of The Foot
Overview
Foot types can be divided into three major groups: the flat foot (Pes Planus), the high arched foot (Pes Valgus) and the normal to low arched foot. A true 'flat foot' is very rare. In fact, less than 5% of the population have flat feet i.e. a foot with no arch present whatsoever and the entire bottom surface of the foot being flat on the ground. About 5-10% of people have a high arched foot. The majority of the population have a normal to low arch. Even though the arches appear to be normal most of us suffer from over-pronation during walking, running and standing, due to the hard, flat unnatural surfaces we walk on, combined with wearing unsupportive footwear. With every step we take the arches flatten and the ankles roll inwards. Pronation itself is not wrong because we need to pronate and supinate as part of our natural gait cycle. Pronation (rolling in) acts as a shock-absorbing mechanism and supination (rolling out) helps to propel our feet forward. Over-pronation occurs when the foot pronates too deep and for too long, not allowing the foot to 'recover' and supinate. Over-pronation hampers our natural walking pattern. It causes an imbalance and leads to wear and tear in several parts of the body with every step we take.
Causes
Over-pronation is very prominent in people who have flexible, flat feet. The framework of the foot begins to collapse, causing the foot to flatten and adding stress to other parts of the foot. As a result, over-pronation, often leads to Plantar Fasciitis, Heel Spurs, Metatarsalgia, Post-tib Tendonitis and/or Bunions. There are many causes of flat feet. Obesity, pregnancy or repetitive pounding on a hard surface can weaken the arch leading to over-pronation. Often people with flat feet do not experience discomfort immediately, and some never suffer from any discomfort at all. However, when symptoms develop and become painful, walking becomes awkward and causes increased strain on the feet and calves.
Symptoms
It is important to note that pronation is not wrong or bad for you. In fact, our feet need to pronate and supinate to achieve proper gait. Pronation (rolling inwards) absorbs shock and supination (rolling outwards) propels our feet forward. It is our body?s natural shock-absorbing mechanism. The problem is over-pronation i.e. the pronation movement goes too deep and lasts for too long, which hinders the foot from recovering and supinating. With every step, excess pronation impedes your natural walking pattern, causing an imbalance in the body and consequent excessive wear and tear in joints, muscles and ligaments. Some common complaints associated with over-pronation include Heel Pain (Plantar Fasciitis) ,Ball of foot pain, Achilles Tendonitis, Shin splints, Knee Pain, Lower Back Pain.
Diagnosis
Look at the wear on your shoes and especially running trainers; if you overpronate it's likely the inside of your shoe will be worn down (or seem crushed if they're soft shoes) from the extra strain.
Non Surgical Treatment
When you see the doctor, he or she will likely perform a complete examination of your feet and watch you walk. The doctor will need to take x-rays to determine the cause of your flat feet. In some cases, further imaging may be needed, especially if your symptoms are severe and sudden in nature. Once you are properly diagnosed, your doctor will create an appropriate treatment plan. There are several options to correct overpronation, such as orthotics. In many cases, overpronation can be treated with non-surgical methods and over-the-counter orthotics. In severe cases, however, custom-made orthotics may work better. Orthotics provide arch support and therefore prevent collapse of the arch with weight bearing. They are made of materials such as spongy rubber or hard plastic. Your doctor will also want to examine your footwear to ensure they fit properly and offer enough medial support. Extra support and stability can be achieved with footwear that has a firm heel counter. If you are experiencing pain, you should be able to use over-the-counter pain medications such as ibuprofen to relieve symptoms.
Prevention
Many of the prevention methods for overpronation-orthotics, for example-can be used interchangeably with treatment methods. If the overpronation is severe, you should seek medical attention from a podiatrist who can cast you for custom-made orthotics. Custom-made orthotics are more expensive, but they last longer and provide support, stability, and balance for the entire foot. You can also talk with a shoe specialist about running shoes that offer extra medial support and firm heel counters. Proper shoes can improve symptoms quickly and prevent them from recurring. Surgery can sometimes help cure and prevent this problem if you suffer from inherited or acquired pes planus deformity. Surgery typically involves stabilizing the bones to improve the foot?s support and function.
Foot types can be divided into three major groups: the flat foot (Pes Planus), the high arched foot (Pes Valgus) and the normal to low arched foot. A true 'flat foot' is very rare. In fact, less than 5% of the population have flat feet i.e. a foot with no arch present whatsoever and the entire bottom surface of the foot being flat on the ground. About 5-10% of people have a high arched foot. The majority of the population have a normal to low arch. Even though the arches appear to be normal most of us suffer from over-pronation during walking, running and standing, due to the hard, flat unnatural surfaces we walk on, combined with wearing unsupportive footwear. With every step we take the arches flatten and the ankles roll inwards. Pronation itself is not wrong because we need to pronate and supinate as part of our natural gait cycle. Pronation (rolling in) acts as a shock-absorbing mechanism and supination (rolling out) helps to propel our feet forward. Over-pronation occurs when the foot pronates too deep and for too long, not allowing the foot to 'recover' and supinate. Over-pronation hampers our natural walking pattern. It causes an imbalance and leads to wear and tear in several parts of the body with every step we take.
Causes
Over-pronation is very prominent in people who have flexible, flat feet. The framework of the foot begins to collapse, causing the foot to flatten and adding stress to other parts of the foot. As a result, over-pronation, often leads to Plantar Fasciitis, Heel Spurs, Metatarsalgia, Post-tib Tendonitis and/or Bunions. There are many causes of flat feet. Obesity, pregnancy or repetitive pounding on a hard surface can weaken the arch leading to over-pronation. Often people with flat feet do not experience discomfort immediately, and some never suffer from any discomfort at all. However, when symptoms develop and become painful, walking becomes awkward and causes increased strain on the feet and calves.
Symptoms
It is important to note that pronation is not wrong or bad for you. In fact, our feet need to pronate and supinate to achieve proper gait. Pronation (rolling inwards) absorbs shock and supination (rolling outwards) propels our feet forward. It is our body?s natural shock-absorbing mechanism. The problem is over-pronation i.e. the pronation movement goes too deep and lasts for too long, which hinders the foot from recovering and supinating. With every step, excess pronation impedes your natural walking pattern, causing an imbalance in the body and consequent excessive wear and tear in joints, muscles and ligaments. Some common complaints associated with over-pronation include Heel Pain (Plantar Fasciitis) ,Ball of foot pain, Achilles Tendonitis, Shin splints, Knee Pain, Lower Back Pain.
Diagnosis
Look at the wear on your shoes and especially running trainers; if you overpronate it's likely the inside of your shoe will be worn down (or seem crushed if they're soft shoes) from the extra strain.
Non Surgical Treatment
When you see the doctor, he or she will likely perform a complete examination of your feet and watch you walk. The doctor will need to take x-rays to determine the cause of your flat feet. In some cases, further imaging may be needed, especially if your symptoms are severe and sudden in nature. Once you are properly diagnosed, your doctor will create an appropriate treatment plan. There are several options to correct overpronation, such as orthotics. In many cases, overpronation can be treated with non-surgical methods and over-the-counter orthotics. In severe cases, however, custom-made orthotics may work better. Orthotics provide arch support and therefore prevent collapse of the arch with weight bearing. They are made of materials such as spongy rubber or hard plastic. Your doctor will also want to examine your footwear to ensure they fit properly and offer enough medial support. Extra support and stability can be achieved with footwear that has a firm heel counter. If you are experiencing pain, you should be able to use over-the-counter pain medications such as ibuprofen to relieve symptoms.
Prevention
Many of the prevention methods for overpronation-orthotics, for example-can be used interchangeably with treatment methods. If the overpronation is severe, you should seek medical attention from a podiatrist who can cast you for custom-made orthotics. Custom-made orthotics are more expensive, but they last longer and provide support, stability, and balance for the entire foot. You can also talk with a shoe specialist about running shoes that offer extra medial support and firm heel counters. Proper shoes can improve symptoms quickly and prevent them from recurring. Surgery can sometimes help cure and prevent this problem if you suffer from inherited or acquired pes planus deformity. Surgery typically involves stabilizing the bones to improve the foot?s support and function.
Do I Care For Calcaneal Apophysitis At Home ?
Overview
Sever's Disease, otherwise known as calcaneal apophysitis is an inflammation of the growth plate in the heel of growing children, typically adolescents. The condition presents as pain in the heel and is caused by repetitive stress to the heel and is thus particularly common in active children. It usually resolves once the bone has completed growth or activity is lessened.
Causes
Mechanically, the heel takes a beating. And the apophyseal bone is located near the point of impact for the heel bone at heel strike and with most weight bearing activities. This includes running, jumping and walking. Heavy impact activities like soccer, football and gymnastics are commonly associated with this problem. In addition to this, there is traction on this apophyseal bone and the associated physeal line of growth cartilage. This traction on the apopysis (island of bone) along with the impact of weight bearing activities can lead to inflammation and pain. Tight Achilles and calf muscles also can contribute to this problem, and why stretching is discussed later.
Symptoms
Pain in the bottom surface and at the back of the heel. Extreme pain when the child places their heel on the ground. The pain is aggravated when running or jumping on hard surfaces. The pain is reduced when the child walks or runs on their toes.
Diagnosis
A doctor or other health professional such as a physiotherapist can diagnose Sever?s disease by asking the young person to describe their symptoms and by conducting a physical examination. In some instances, an x-ray may be necessary to rule out other causes of heel pain, such as heel fractures. Sever?s disease does not show on an x-ray because the damage is in the cartilage.
Non Surgical Treatment
Treatment revolves around decreasing activity. Usual treatment has been putting children in a boot in slight equinus, or a cast with the foot in slight equinus, thereby decreasing the tension on the heel cord, which in turn pulls on the growth plate at the heel. As the pain resolves, children are allowed to go back to full activities. Complete resolution may be delayed until growth of the foot is complete (when the growth plate fuses to the rest of the bone of the heel). A soft cushioning heel raise is really important (this reduces the pull from the calf muscles on the growth plate and increases the shock absorption, so the growth plate is not knocked around as much). The use of an ice pack after activity for 20mins is often useful for calcaneal apophysitis, this should be repeated 2 to 3 times a day. As a pronated foot is common in children with this problem, a discussion regarding the use of long term foot orthotics may be important. If the symptoms are bad enough and are not responding to these measures, medication to help with inflammation may be needed. In some cases the lower limb may need to be put in a cast for 2-6 weeks to give it a good chance to heal.
Recovery
If the child has a pronated foot, a flat or high arch, or another condition that increases the risk of Sever's disease, the doctor might recommend special shoe inserts, called orthotic devices, such as heel pads that cushion the heel as it strikes the ground, heel lifts that reduce strain on the Achilles tendon by raising the heel, arch supports that hold the heel in an ideal position. If a child is overweight or obese, the doctor will probably also recommend weight loss to decrease pressure on the heel. The risk of recurrence goes away on its own when foot growth is complete and the growth plate has fused to the rest of the heel bone, usually around age 15.
Sever's Disease, otherwise known as calcaneal apophysitis is an inflammation of the growth plate in the heel of growing children, typically adolescents. The condition presents as pain in the heel and is caused by repetitive stress to the heel and is thus particularly common in active children. It usually resolves once the bone has completed growth or activity is lessened.
Causes
Mechanically, the heel takes a beating. And the apophyseal bone is located near the point of impact for the heel bone at heel strike and with most weight bearing activities. This includes running, jumping and walking. Heavy impact activities like soccer, football and gymnastics are commonly associated with this problem. In addition to this, there is traction on this apophyseal bone and the associated physeal line of growth cartilage. This traction on the apopysis (island of bone) along with the impact of weight bearing activities can lead to inflammation and pain. Tight Achilles and calf muscles also can contribute to this problem, and why stretching is discussed later.
Symptoms
Pain in the bottom surface and at the back of the heel. Extreme pain when the child places their heel on the ground. The pain is aggravated when running or jumping on hard surfaces. The pain is reduced when the child walks or runs on their toes.
Diagnosis
A doctor or other health professional such as a physiotherapist can diagnose Sever?s disease by asking the young person to describe their symptoms and by conducting a physical examination. In some instances, an x-ray may be necessary to rule out other causes of heel pain, such as heel fractures. Sever?s disease does not show on an x-ray because the damage is in the cartilage.
Non Surgical Treatment
Treatment revolves around decreasing activity. Usual treatment has been putting children in a boot in slight equinus, or a cast with the foot in slight equinus, thereby decreasing the tension on the heel cord, which in turn pulls on the growth plate at the heel. As the pain resolves, children are allowed to go back to full activities. Complete resolution may be delayed until growth of the foot is complete (when the growth plate fuses to the rest of the bone of the heel). A soft cushioning heel raise is really important (this reduces the pull from the calf muscles on the growth plate and increases the shock absorption, so the growth plate is not knocked around as much). The use of an ice pack after activity for 20mins is often useful for calcaneal apophysitis, this should be repeated 2 to 3 times a day. As a pronated foot is common in children with this problem, a discussion regarding the use of long term foot orthotics may be important. If the symptoms are bad enough and are not responding to these measures, medication to help with inflammation may be needed. In some cases the lower limb may need to be put in a cast for 2-6 weeks to give it a good chance to heal.
Recovery
If the child has a pronated foot, a flat or high arch, or another condition that increases the risk of Sever's disease, the doctor might recommend special shoe inserts, called orthotic devices, such as heel pads that cushion the heel as it strikes the ground, heel lifts that reduce strain on the Achilles tendon by raising the heel, arch supports that hold the heel in an ideal position. If a child is overweight or obese, the doctor will probably also recommend weight loss to decrease pressure on the heel. The risk of recurrence goes away on its own when foot growth is complete and the growth plate has fused to the rest of the heel bone, usually around age 15.
Will Adult Aquired Flat Foot Involve Surgical Teatment ?
Overview
Adult-acquired flatfoot is a challenging condition to treat. It is defined as a symptomatic, progressive deformity of the foot caused by loss of supportive structures of the medial arch. It is becoming increasingly frequent with the aging population and the obesity epidemic. Patients commonly try to lose weight by exercising to improve the condition. This often leads to worsening of symptoms and progression of the disorder. Early recognition of this complex disorder is essential, if chronic pain and surgery are to be avoided. 
Causes
As discussed above, many different problems can create a painful flatfoot. Damage to the posterior tibial tendon is the most common cause of AAFD. The posterior tibial tendon is one of the most important tendons of the leg. It starts at a muscle in the calf, travels down the inside of the lower leg and attaches to the bones on the inside of the foot. The main function of this tendon is to support the arch of your foot when you walk. If the tendon becomes inflamed or torn, the arch will slowly collapse. Women and people over 40 are more likely to develop problems with the posterior tibial tendon. Other risk factors include obesity, diabetes, and hypertension. Having flat feet since childhood increases the risk of developing a tear in the posterior tibial tendon. In addition, people who are involved in high impact sports, such as basketball, tennis, or soccer, may have tears of the tendon from repetitive use. Inflammatory arthritis, such as rheumatoid arthritis, can cause a painful flatfoot. This type of arthritis attacks not only the cartilage in the joints, but also the ligaments that support the foot. Inflammatory arthritis not only causes pain, but also causes the foot to change shape and become flat. The arthritis can affect the back of the foot or the middle of foot, both of which can result in a fallen arch. An injury to the tendons or ligaments in the foot can cause the joints to fall out of alignment. The ligaments support the bones and prevent them from moving. If the ligaments are torn, the foot will become flat and painful. This more commonly occurs in the middle of the foot (Lisfranc injury), but can also occur in the back of the foot. Injuries to tendons of the foot can occur either in one instance (traumatically) or with repeated use over time (overuse injury). Regardless of the cause, if tendon function is altered, the forces that are transmitted across joints in the foot are changed and this can lead to increased stress on joint cartilage and ligaments. In addition to tendon and ligament injuries, fractures and dislocations of the bones in the midfoot can also lead to a flatfoot deformity. People with diabetes or with nerve problems that limits normal feeling in the feet, can have collapse of the arch or of the entire foot. This type of arch collapse is typically more severe than that seen in patients with normal feeling in their feet. In addition to the ligaments not holding the bones in place, the bones themselves can sometimes fracture and disintegrate without the patient feeling any pain. This may result in a severely deformed foot that is very challenging to correct with surgery. Special shoes or braces are the best method for dealing with this problem.
Symptoms
At first you may notice pain and swelling along the medial (big toe) side of the foot. This is where the posterior tibialis tendon travels from the back of the leg under the medial ankle bone to the foot. As the condition gets worse, tendon failure occurs and the pain gets worse. Some patients experience pain along the lateral (outside) edge of the foot, too. You may find that your feet hurt at the end of the day or after long periods of standing. Some people with this condition have trouble rising up on their toes. They may be unable to participate fully in sports or other recreational activities.
Diagnosis
Posterior Tibial Tendon Dysfunction is diagnosed with careful clinical observation of the patient?s gait (walking), range of motion testing for the foot and ankle joints, and diagnostic imaging. People with flatfoot deformity walk with the heel angled outward, also called over-pronation. Although it is normal for the arch to impact the ground for shock absorption, people with PTTD have an arch that fully collapses to the ground and does not reform an arch during the entire gait period. After evaluating the ambulation pattern, the foot and ankle range of motion should be tested. Usually the affected foot will have decreased motion to the ankle joint and the hindfoot. Muscle strength may also be weaker as well. An easy test to perform for PTTD is the single heel raise where the patient is asked to raise up on the ball of his or her effected foot. A normal foot type can lift up on the toes without pain and the heel will invert slightly once the person has fully raised the heel up during the test. In early phases of PTTD the patient may be able to lift up the heel but the heel will not invert. An elongated or torn posterior tibial tendon, which is a mid to late finding of PTTD, will prohibit the patient from fully rising up on the heel and will cause intense pain to the arch. Finally diagnostic imaging, although used alone cannot diagnose PTTD, can provide additional information for an accurate diagnosis of flatfoot deformity. Xrays of the foot can show the practitioner important angular relationships of the hindfoot and forefoot which help diagnose flatfoot deformity. Most of the time, an MRI is not needed to diagnose PTTD but is a tool that should be considered in advanced cases of flatfoot deformity. If a partial tear of the posterior tibial tendon is of concern, then an MRI can show the anatomic location of the tear and the extensiveness of the injury.
Non surgical Treatment
Get treated early. There is no recommended home treatment. While in stage one of the deformity, rest, a cast, and anti-inflammatory therapy can help you find relief. This treatment is followed by creating custom-molded foot orthoses and orthopedic footwear. These customized items are critical in maintaining the stability of the foot and ankle. Once the tendon has stretched and deformity is visible, the chances of success for non-surgical treatment are significantly lower. In a small percentage of patients, total immobilization may arrest the progression of the deformity. A long-term brace known as an ankle foot orthosis is required to keep the deformity from progressing. The Richie Brace, a type of ankle foot orthosis, shows significant success as a treatment for stage two posterior tibial dysfunction. It is a sport-style brace connected to a custom corrected foot orthodic that fits into most lace-up footwear (including athletic shoes). It is also light weight and more cosmetically appealing than traditionally prescribed ankle foot orthosis. The Arizona Brace, California Brace or Gauntlet Brace may also be recommended depending on your needs. 
Surgical Treatment
Flatfoot reconstruction (osteotomy). This is often recommended for flexible flatfoot condition. Flatfoot reconstruction involves cutting and shifting the heel bone into a more neutral position, transferring the tendon used to flex the lesser toes (all but the big toe) to strengthen the posterior tibial tendon, and lengthening the calf muscle. Fusion (also known as triple arthrodesis). Fusion involves fusing, or making stiff, three joints in the back of the foot the subtalar, talonavicular, and calcaneocuboid joints, to realign the foot and give it a more natural shape. Pins or screws hold the area in place until it heals. Fusion is often recommended for a rigid flatfoot deformity or evidence of arthritis. Both of these surgeries can provide excellent pain relief and correction.
Severe Arch Pain In Foot
Overview
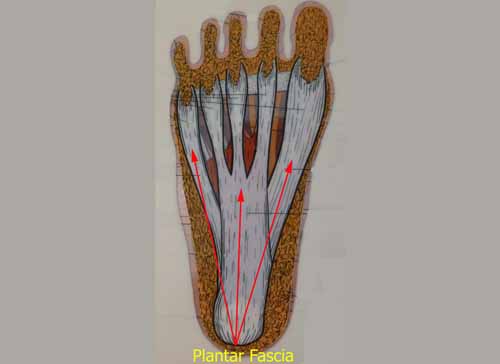
We all experience sore arches now and again after a long hike, standing in a long line or walking from one end to the other of a big shopping mall. It's normal for feet to get tired out sometimes, and there's usually no need to worry unless the pain persists. If you're turning to the web because it's dawning on you that your arches are sore several days a week, or maybe even every day, you're doing a smart thing. Chronic pain in the arches can actually be a symptom of a significant underlying condition called Plantar Fasciitis that requires attention and treatment to prevent it from worsening. This article will quickly point out what you need to know about arch pain and Plantar Fasciitis and provide you with resources for learning how to recover.

Causes
At the other end of the spectrum, yet within the same category of congenital flat foot, exist several rare, more severe forms of flat foot. These severe conditions include Vertical Talus, Congenital Calcaneal Valgus, and Tarsal Coalitions - all of which are more rigid (no arch with or without weight on the foot) and definitely symptomatic. Luckily, these are much less common, but can usually be identified by specialists at the time of presentation and treated appropriately. The second category, acquired flat foot, develops over time, rather than at birth. Many different factors can contribute to the development of flat feet. These include the types of shoes a child wears, a child's sitting or sleeping positions, compensation for other abnormalities further up the leg, or more severe factors such as rupture of ligaments or tendons in the foot. Very commonly, the reason for flat feet is that the foot is compensating for a tight Achilles tendon. If the Achilles tendon is tight, then it causes the foot to point down, or to plantarflex (as occurs when stepping on the accelerator of your car). Even minimal amounts of plantarflexion can simulate a longer leg on that particular side, assuming that the other foot is in the normal position. The body therefore tries to compensate by pronating, or flattening out the arch, thereby making up for the perceived extra length on the affected side.
Symptoms
The most common symptoms of plantar fasciitis include pain on the bottom of the foot near the heel, pain with the first few steps after getting out of bed in the morning, or after a long period of rest, such as after a long car ride. The pain subsides after a few minutes of walking. Greater pain after (not during) exercise or activity.
Diagnosis
Flat feet are easy to identify while standing or walking. When someone with flat feet stands, their inner foot or arch flattens and their foot may roll over to the inner side. This is known as overpronation. To see whether your foot overpronates, stand on tiptoes or push your big toe back as far as possible. If the arch of your foot doesn't appear, your foot is likely to overpronate when you walk or run. It can be difficult to tell whether a child has flat feet because their arches may not fully develop until they're 10 years of age.
Non Surgical Treatment
Flat feet in a child do not need treatment if they are not causing pain or walking problems. Your child's feet will grow and develop the same, whether special shoes, shoe inserts, heel cups, or wedges are used. Your child may walk barefoot, run or jump, or do any other activity without making the flat feet worse. In older children and adults, flexible flat feet that do not cause pain or walking problems do not need further treatment. If you have pain due to flexible flat feet, the following may help. An arch-support (orthotic) that you put in your shoe. You can buy this at the store or have it custom-made. Special shoes. Rigid or painful flat feet need to be checked by a health care provider. The treatment depends on the cause of the flat feet. For tarsal coalition, treatment starts with rest and possibly a cast. Surgery may be needed if pain does not improve. In more severe cases, surgery may be needed to clean or repair the tendon, fuse joints in the foot into a corrected position. Flat feet in older adults can be treated with pain relievers, orthotics, and sometimes surgery.
Surgical Treatment
The procedure involves cutting and shifting the bone, and then performing a tendon transfer. First, the surgeon performs a calcaneal osteotomy, cutting the heel bone and shifting it into the correct position. Second, the surgeon transfers the tendon. Reroute the flexor digitorum to replace the troublesome posterior tibial tendon. Finally, the surgeon typically performs one or more fine-tuning procedures that address the patient?s specific foot deformity. Often, the surgeon will lengthen the Achilles tendon because it is common for the mispositioned foot to cause the Achilles to tighten. Occasionally, to increase the arch, the surgeon performs another osteotomy of one of the bones of the midfoot. Occasionally, to point the foot in a straightforward direction, the surgeon performs another osteotomy of the outside portion of the calcaneus.
Stretching Exercises
Plantar Fasciitis stretches can be incorporated into a comprehensive treatment regime which may involve: ice, heel wedge support, taping, massage, muscle strengthening, orthotic inserts for shoes, topical anti inflammatory gel or oral medication and/or corticosteroid injections. If you suspect you may have Plantar Fasciitis seek accurate diagnosis and treatment from a health professional to ensure a correct diagnosis and reduce the likelihood of developing chronic foot pain. Treatment interventions may be provided by your Physical Therapist, Podiatrist and/or doctor.
We all experience sore arches now and again after a long hike, standing in a long line or walking from one end to the other of a big shopping mall. It's normal for feet to get tired out sometimes, and there's usually no need to worry unless the pain persists. If you're turning to the web because it's dawning on you that your arches are sore several days a week, or maybe even every day, you're doing a smart thing. Chronic pain in the arches can actually be a symptom of a significant underlying condition called Plantar Fasciitis that requires attention and treatment to prevent it from worsening. This article will quickly point out what you need to know about arch pain and Plantar Fasciitis and provide you with resources for learning how to recover.
Causes
At the other end of the spectrum, yet within the same category of congenital flat foot, exist several rare, more severe forms of flat foot. These severe conditions include Vertical Talus, Congenital Calcaneal Valgus, and Tarsal Coalitions - all of which are more rigid (no arch with or without weight on the foot) and definitely symptomatic. Luckily, these are much less common, but can usually be identified by specialists at the time of presentation and treated appropriately. The second category, acquired flat foot, develops over time, rather than at birth. Many different factors can contribute to the development of flat feet. These include the types of shoes a child wears, a child's sitting or sleeping positions, compensation for other abnormalities further up the leg, or more severe factors such as rupture of ligaments or tendons in the foot. Very commonly, the reason for flat feet is that the foot is compensating for a tight Achilles tendon. If the Achilles tendon is tight, then it causes the foot to point down, or to plantarflex (as occurs when stepping on the accelerator of your car). Even minimal amounts of plantarflexion can simulate a longer leg on that particular side, assuming that the other foot is in the normal position. The body therefore tries to compensate by pronating, or flattening out the arch, thereby making up for the perceived extra length on the affected side.
Symptoms
The most common symptoms of plantar fasciitis include pain on the bottom of the foot near the heel, pain with the first few steps after getting out of bed in the morning, or after a long period of rest, such as after a long car ride. The pain subsides after a few minutes of walking. Greater pain after (not during) exercise or activity.
Diagnosis
Flat feet are easy to identify while standing or walking. When someone with flat feet stands, their inner foot or arch flattens and their foot may roll over to the inner side. This is known as overpronation. To see whether your foot overpronates, stand on tiptoes or push your big toe back as far as possible. If the arch of your foot doesn't appear, your foot is likely to overpronate when you walk or run. It can be difficult to tell whether a child has flat feet because their arches may not fully develop until they're 10 years of age.
Non Surgical Treatment
Flat feet in a child do not need treatment if they are not causing pain or walking problems. Your child's feet will grow and develop the same, whether special shoes, shoe inserts, heel cups, or wedges are used. Your child may walk barefoot, run or jump, or do any other activity without making the flat feet worse. In older children and adults, flexible flat feet that do not cause pain or walking problems do not need further treatment. If you have pain due to flexible flat feet, the following may help. An arch-support (orthotic) that you put in your shoe. You can buy this at the store or have it custom-made. Special shoes. Rigid or painful flat feet need to be checked by a health care provider. The treatment depends on the cause of the flat feet. For tarsal coalition, treatment starts with rest and possibly a cast. Surgery may be needed if pain does not improve. In more severe cases, surgery may be needed to clean or repair the tendon, fuse joints in the foot into a corrected position. Flat feet in older adults can be treated with pain relievers, orthotics, and sometimes surgery.
Surgical Treatment
The procedure involves cutting and shifting the bone, and then performing a tendon transfer. First, the surgeon performs a calcaneal osteotomy, cutting the heel bone and shifting it into the correct position. Second, the surgeon transfers the tendon. Reroute the flexor digitorum to replace the troublesome posterior tibial tendon. Finally, the surgeon typically performs one or more fine-tuning procedures that address the patient?s specific foot deformity. Often, the surgeon will lengthen the Achilles tendon because it is common for the mispositioned foot to cause the Achilles to tighten. Occasionally, to increase the arch, the surgeon performs another osteotomy of one of the bones of the midfoot. Occasionally, to point the foot in a straightforward direction, the surgeon performs another osteotomy of the outside portion of the calcaneus.
Stretching Exercises
Plantar Fasciitis stretches can be incorporated into a comprehensive treatment regime which may involve: ice, heel wedge support, taping, massage, muscle strengthening, orthotic inserts for shoes, topical anti inflammatory gel or oral medication and/or corticosteroid injections. If you suspect you may have Plantar Fasciitis seek accurate diagnosis and treatment from a health professional to ensure a correct diagnosis and reduce the likelihood of developing chronic foot pain. Treatment interventions may be provided by your Physical Therapist, Podiatrist and/or doctor.
Are Fallen Arches Flat Feet?
Overview
Fallen arches, or flatfoot, is a condition in which the arch on the inside of the foot is flat and the entire sole of the foot rests on the ground. It affects about 40% of the general population. Although flat feet in themselves are not usually problematic, they can create problems in the feet, hips, ankles and knees. Pain may be experienced in the lower back if there are alignment problems and if the individual is engaged in a lot of heavy, high impact activities that put stress on the bones and muscles in the lower legs. The arches of most individuals are fully developed by the age of 12 to 13. While some people are born with flat arches, for others the arches fall over time. The tibial tendon, which runs along the inside of the ankle from above the ankle to the arch, can weaken with age and with heavy activity. The posterior tendon, main support structure for the arch, can become inflamed (tendonitis) or even tear if overloaded. For women, wearing high heels can affect the Achilles tendon and alter the structure and function of the ankle. The posterior tibial tendon may compensate for this stress and break down, causing the arches to fall. Obesity is another contributing factor, as well as a serious injury to the ankle or foot, arthritis and bad circulation such as occurs with diabetes.
Causes
Footwear: shoes which limit toe movement; high heels. Barefoot walking may be protective. A tight Achilles tendon or calf muscles (heel cord contracture). This may help to cause Pes Planus, or may contribute to symptoms such as foot pain when there is existing Pes Planus. Obesity. Other bony abnormalities, eg rotational deformities, tibial abnormalities, coalition (fusion) of tarsal bones, equinus deformity. Ligamentous laxity, eg familial, Marfan's syndrome, Ehlers-Danlos syndrome, Down's syndrome. Other factors causing foot pronation, eg hip abductor weakness and genu valgum.
Symptoms
Flat feet don't usually cause problems, but they can put a strain on your muscles and ligaments (ligaments link two bones together at a joint). This may cause pain in your legs when you walk. If you have flat feet, you may experience pain in any of the following areas, the inside of your ankle, the arch of your foot, the outer side of your foot, the calf, the knee, hip or back. Some people with flat feet find that their weight is distributed unevenly, particularly if their foot rolls inwards too much (overpronates). If your foot overpronates, your shoes are likely to wear out quickly. Overpronation can also damage your ankle joint and Achilles tendon (the large tendon at the back of your ankle).
Diagnosis
It is important for people with foot pain to know if they have flat feet. The following tests can help you determine your arch type. When you get out of a swimming pool, look at your footprint on the concrete. The front of the foot will be joined to the heel by a strip. If your foot is flat, then the strip is the same width as the front of the foot, creating a footprint that looks like a stretched out pancake. With a normal arch, the strip is about half the width of the front of the foot. If you have a high arch, only a thin strip connects the front of the foot with the heel. Put your shoes on a flat table and view them at eye level from behind. See if the sole is worn evenly. A flat foot will cause more wear on the inside of the sole, especially in the heel area. The shoe will easily rock side to side. A flat foot will also cause the upper part of the shoe to lean inward over the sole. Both shoes should wear about the same way. If you have pain in one foot, you should make sure you don't have a fallen arch on that side. There are two good tests you can perform at home to detect this problem. Place your fingertips on a wall that you are directly facing and stand on your tiptoes on one foot. If you can't do it, a fallen arch may be the culprit. Stand with your feet parallel. Have someone stand in back of you and look at your feet from behind. You can also do it yourself if you stand with your back to a mirror. Normally, only the pinky toe is visible from behind. If one foot is flatter than the other, the 4th and sometimes the 3rd toe on that foot can also be seen.
Non Surgical Treatment
Most patients can be treated without surgery using orthotics, supportive shoes and braces. Because of the progressive nature of PTTD, early treatment is advised. If treated early enough, your symptoms may resolve without the need for surgery and progression of your condition can be arrested. In contrast, untreated PTTD could leave you with an extremely flat foot, painful arthritis in the foot and ankle, and increasing limitations on walking, running, or other activities.
Surgical Treatment

Common indications for surgery are cerebral palsy with an equinovalgus foot, to prevent progression and breakdown of the midfoot. Rigid and painful Pes Planus. To prevent progression, eg with a Charcot joint. Tibialis posterior dysfunction, where non-surgical treatment is unsuccessful. Possible surgical procedures include Achilles tendon lengthening. Calcaneal osteotomy, to re-align the hindfoot. Reconstruction of the tibialis posterior tendon. For severe midfoot collapse of the arch, triple arthrodesis may be indicated.
After Care
Patients may go home the day of surgery or they may require an overnight hospital stay. The leg will be placed in a splint or cast and should be kept elevated for the first two weeks. At that point, sutures are removed. A new cast or a removable boot is then placed. It is important that patients do not put any weight on the corrected foot for six to eight weeks following the operation. Patients may begin bearing weight at eight weeks and usually progress to full weightbearing by 10 to 12 weeks. For some patients, weightbearing requires additional time. After 12 weeks, patients commonly can transition to wearing a shoe. Inserts and ankle braces are often used. Physical therapy may be recommended. There are complications that relate to surgery in general. These include the risks associated with anesthesia, infection, damage to nerves and blood vessels, and bleeding or blood clots. Complications following flatfoot surgery may include wound breakdown or nonunion (incomplete healing of the bones). These complications often can be prevented with proper wound care and rehabilitation. Occasionally, patients may notice some discomfort due to prominent hardware. Removal of hardware can be done at a later time if this is an issue. The overall complication rates for flatfoot surgery are low.
Fallen arches, or flatfoot, is a condition in which the arch on the inside of the foot is flat and the entire sole of the foot rests on the ground. It affects about 40% of the general population. Although flat feet in themselves are not usually problematic, they can create problems in the feet, hips, ankles and knees. Pain may be experienced in the lower back if there are alignment problems and if the individual is engaged in a lot of heavy, high impact activities that put stress on the bones and muscles in the lower legs. The arches of most individuals are fully developed by the age of 12 to 13. While some people are born with flat arches, for others the arches fall over time. The tibial tendon, which runs along the inside of the ankle from above the ankle to the arch, can weaken with age and with heavy activity. The posterior tendon, main support structure for the arch, can become inflamed (tendonitis) or even tear if overloaded. For women, wearing high heels can affect the Achilles tendon and alter the structure and function of the ankle. The posterior tibial tendon may compensate for this stress and break down, causing the arches to fall. Obesity is another contributing factor, as well as a serious injury to the ankle or foot, arthritis and bad circulation such as occurs with diabetes.
Causes
Footwear: shoes which limit toe movement; high heels. Barefoot walking may be protective. A tight Achilles tendon or calf muscles (heel cord contracture). This may help to cause Pes Planus, or may contribute to symptoms such as foot pain when there is existing Pes Planus. Obesity. Other bony abnormalities, eg rotational deformities, tibial abnormalities, coalition (fusion) of tarsal bones, equinus deformity. Ligamentous laxity, eg familial, Marfan's syndrome, Ehlers-Danlos syndrome, Down's syndrome. Other factors causing foot pronation, eg hip abductor weakness and genu valgum.
Symptoms
Flat feet don't usually cause problems, but they can put a strain on your muscles and ligaments (ligaments link two bones together at a joint). This may cause pain in your legs when you walk. If you have flat feet, you may experience pain in any of the following areas, the inside of your ankle, the arch of your foot, the outer side of your foot, the calf, the knee, hip or back. Some people with flat feet find that their weight is distributed unevenly, particularly if their foot rolls inwards too much (overpronates). If your foot overpronates, your shoes are likely to wear out quickly. Overpronation can also damage your ankle joint and Achilles tendon (the large tendon at the back of your ankle).
Diagnosis
It is important for people with foot pain to know if they have flat feet. The following tests can help you determine your arch type. When you get out of a swimming pool, look at your footprint on the concrete. The front of the foot will be joined to the heel by a strip. If your foot is flat, then the strip is the same width as the front of the foot, creating a footprint that looks like a stretched out pancake. With a normal arch, the strip is about half the width of the front of the foot. If you have a high arch, only a thin strip connects the front of the foot with the heel. Put your shoes on a flat table and view them at eye level from behind. See if the sole is worn evenly. A flat foot will cause more wear on the inside of the sole, especially in the heel area. The shoe will easily rock side to side. A flat foot will also cause the upper part of the shoe to lean inward over the sole. Both shoes should wear about the same way. If you have pain in one foot, you should make sure you don't have a fallen arch on that side. There are two good tests you can perform at home to detect this problem. Place your fingertips on a wall that you are directly facing and stand on your tiptoes on one foot. If you can't do it, a fallen arch may be the culprit. Stand with your feet parallel. Have someone stand in back of you and look at your feet from behind. You can also do it yourself if you stand with your back to a mirror. Normally, only the pinky toe is visible from behind. If one foot is flatter than the other, the 4th and sometimes the 3rd toe on that foot can also be seen.
Non Surgical Treatment
Most patients can be treated without surgery using orthotics, supportive shoes and braces. Because of the progressive nature of PTTD, early treatment is advised. If treated early enough, your symptoms may resolve without the need for surgery and progression of your condition can be arrested. In contrast, untreated PTTD could leave you with an extremely flat foot, painful arthritis in the foot and ankle, and increasing limitations on walking, running, or other activities.
Surgical Treatment
Common indications for surgery are cerebral palsy with an equinovalgus foot, to prevent progression and breakdown of the midfoot. Rigid and painful Pes Planus. To prevent progression, eg with a Charcot joint. Tibialis posterior dysfunction, where non-surgical treatment is unsuccessful. Possible surgical procedures include Achilles tendon lengthening. Calcaneal osteotomy, to re-align the hindfoot. Reconstruction of the tibialis posterior tendon. For severe midfoot collapse of the arch, triple arthrodesis may be indicated.
After Care
Patients may go home the day of surgery or they may require an overnight hospital stay. The leg will be placed in a splint or cast and should be kept elevated for the first two weeks. At that point, sutures are removed. A new cast or a removable boot is then placed. It is important that patients do not put any weight on the corrected foot for six to eight weeks following the operation. Patients may begin bearing weight at eight weeks and usually progress to full weightbearing by 10 to 12 weeks. For some patients, weightbearing requires additional time. After 12 weeks, patients commonly can transition to wearing a shoe. Inserts and ankle braces are often used. Physical therapy may be recommended. There are complications that relate to surgery in general. These include the risks associated with anesthesia, infection, damage to nerves and blood vessels, and bleeding or blood clots. Complications following flatfoot surgery may include wound breakdown or nonunion (incomplete healing of the bones). These complications often can be prevented with proper wound care and rehabilitation. Occasionally, patients may notice some discomfort due to prominent hardware. Removal of hardware can be done at a later time if this is an issue. The overall complication rates for flatfoot surgery are low.
How To Get Rid Of Bunions At Home
Overview

When your big toe is angled towards the second toe, the deformity is called a bunion (hallux valgus). This causes a bump on the side at the base of the big toe. In addition there is often thickening of the skin and tissues next to the affected joint. The thickened skin and tissues may become inflamed, swollen and painful. Sometimes a fluid-filled sac (bursa) develops over the joint.
Causes
The exact cause of bunions is unknown, but they tend to run in families. Wearing badly fitting shoes is thought to make bunions worse. It's also thought that bunions are more likely to occur in people with unusually flexible joints, which is why bunions sometimes occur in children. In some cases, certain health conditions, such as rheumatoid arthritis and gout, may also be responsible.
Symptoms
Alteration in alignment of the first toe. Pain in the 1st toe joint with movement. Restriction in range of demi pointe. Inflammation of the 1st toe joint. Rotation of the big toe so that the nail no longer faces upwards. Occasionally bruising of the toe nail occurs.
Diagnosis
People with bunions may be concerned about the changing appearance of their feet, but it is usually the pain caused by the condition that leads them to consult their doctor. The doctor will evaluate any symptoms experienced and examine the affected foot for joint enlargement, tissue swelling and/or tenderness. They will also assess any risk factors for the condition and will ask about family history. An x-ray of the foot is usually recommended so that the alignment of big toe joint can be assessed. This would also allow any other conditions that may be affecting the joint, such as arthritis, to be seen.
Non Surgical Treatment
Nonsurgical treatments that may relieve the pain and pressure of a bunion include changing shoes. Wear roomy, comfortable shoes that provide plenty of space for your toes. Padding and taping or splinting. Your doctor can help you tape and pad your foot in a normal position. This can reduce stress on the bunion and alleviate your pain. Medications. Acetaminophen (Tylenol, others), ibuprofen (Advil, Motrin IB, others) or naproxen (Aleve) can help you control the pain of a bunion. Cortisone injections also can be helpful. Shoe inserts. Padded shoe inserts can help distribute pressure evenly when you move your feet, reducing your symptoms and preventing your bunion from getting worse. Over-the-counter arch supports can provide relief for some people, although others may require prescription orthotic devices. Applying ice. Icing your bunion after you've been on your feet too long can help relieve soreness and inflammation.

Surgical Treatment
Research shows that 85% of people who have bunion corrections are satisfied with the results. However, a number of problems can arise. The big toe is usually stiffer than before. For most people this does not matter, but for athletes or dancers it is very important. As mentioned before, the big toe is slightly weaker with a bunion, and this transfers weight onto the ball of the foot. After bunion surgery, this transfer of weight can increase. Therefore, if you have pain under the ball of the foot ("metatarsalgia") it may be worse after bunion surgery, and it may also develop for the first time. Careful surgical technique can reduce this risk, but it cannot avoid it completely. Most people who develop metatarsalgia are comfortable with a simple insole in the shoe but occasionally surgery is required. In some people the big toe slowly tilts back toward the original position and occasionally this is bad enough to need to have the operation redone. On the other hand, the toe can tilt the other way, though much more rarely. Again, occasionally this is bad enough to need to have the operation redone. Infections in the wound, plaster problems and minor damage to the nerves of the toe can occur in any foot surgery. Usually these are minor problems that get better quickly. This may sound like a lot of possible problems, but in fact most people do not get them and are satisfied with their bunion surgery. However, this may help you to see how important it is to have any bunion surgery carried out by a properly trained and experienced foot and ankle surgeon.
Prevention
Because bunions develop slowly, taking care of your feet during childhood and early adulthood can pay off later in life. Keep track of the shape of your feet as they develop over time, especially if foot problems run in your family. Exercising your feet can strengthen them. Learn to pick up small objects, like a pencil or pebble, with your toes. Wear shoes that fit properly and don't cramp or pinch your toes. Women should avoid shoes with very high heels or pointed toes.
When your big toe is angled towards the second toe, the deformity is called a bunion (hallux valgus). This causes a bump on the side at the base of the big toe. In addition there is often thickening of the skin and tissues next to the affected joint. The thickened skin and tissues may become inflamed, swollen and painful. Sometimes a fluid-filled sac (bursa) develops over the joint.
Causes
The exact cause of bunions is unknown, but they tend to run in families. Wearing badly fitting shoes is thought to make bunions worse. It's also thought that bunions are more likely to occur in people with unusually flexible joints, which is why bunions sometimes occur in children. In some cases, certain health conditions, such as rheumatoid arthritis and gout, may also be responsible.
Symptoms
Alteration in alignment of the first toe. Pain in the 1st toe joint with movement. Restriction in range of demi pointe. Inflammation of the 1st toe joint. Rotation of the big toe so that the nail no longer faces upwards. Occasionally bruising of the toe nail occurs.
Diagnosis
People with bunions may be concerned about the changing appearance of their feet, but it is usually the pain caused by the condition that leads them to consult their doctor. The doctor will evaluate any symptoms experienced and examine the affected foot for joint enlargement, tissue swelling and/or tenderness. They will also assess any risk factors for the condition and will ask about family history. An x-ray of the foot is usually recommended so that the alignment of big toe joint can be assessed. This would also allow any other conditions that may be affecting the joint, such as arthritis, to be seen.
Non Surgical Treatment
Nonsurgical treatments that may relieve the pain and pressure of a bunion include changing shoes. Wear roomy, comfortable shoes that provide plenty of space for your toes. Padding and taping or splinting. Your doctor can help you tape and pad your foot in a normal position. This can reduce stress on the bunion and alleviate your pain. Medications. Acetaminophen (Tylenol, others), ibuprofen (Advil, Motrin IB, others) or naproxen (Aleve) can help you control the pain of a bunion. Cortisone injections also can be helpful. Shoe inserts. Padded shoe inserts can help distribute pressure evenly when you move your feet, reducing your symptoms and preventing your bunion from getting worse. Over-the-counter arch supports can provide relief for some people, although others may require prescription orthotic devices. Applying ice. Icing your bunion after you've been on your feet too long can help relieve soreness and inflammation.
Surgical Treatment
Research shows that 85% of people who have bunion corrections are satisfied with the results. However, a number of problems can arise. The big toe is usually stiffer than before. For most people this does not matter, but for athletes or dancers it is very important. As mentioned before, the big toe is slightly weaker with a bunion, and this transfers weight onto the ball of the foot. After bunion surgery, this transfer of weight can increase. Therefore, if you have pain under the ball of the foot ("metatarsalgia") it may be worse after bunion surgery, and it may also develop for the first time. Careful surgical technique can reduce this risk, but it cannot avoid it completely. Most people who develop metatarsalgia are comfortable with a simple insole in the shoe but occasionally surgery is required. In some people the big toe slowly tilts back toward the original position and occasionally this is bad enough to need to have the operation redone. On the other hand, the toe can tilt the other way, though much more rarely. Again, occasionally this is bad enough to need to have the operation redone. Infections in the wound, plaster problems and minor damage to the nerves of the toe can occur in any foot surgery. Usually these are minor problems that get better quickly. This may sound like a lot of possible problems, but in fact most people do not get them and are satisfied with their bunion surgery. However, this may help you to see how important it is to have any bunion surgery carried out by a properly trained and experienced foot and ankle surgeon.
Prevention
Because bunions develop slowly, taking care of your feet during childhood and early adulthood can pay off later in life. Keep track of the shape of your feet as they develop over time, especially if foot problems run in your family. Exercising your feet can strengthen them. Learn to pick up small objects, like a pencil or pebble, with your toes. Wear shoes that fit properly and don't cramp or pinch your toes. Women should avoid shoes with very high heels or pointed toes.